It’s been my pleasure to host Laurie this week. In her final post she gives a brief overview of medicine during the 1860’s. This is great information for any historical writer. Thanks Laurie for all of your hard work!
THE STATE OF MEDICINE IN THE 1860’S
A writer always wants to make her hero an admirable person, perhaps even exceptional for his time, but still realistic. Nowhere is this more of a challenge, I believe, than when one’s hero is a doctor in the past.
Medical colleges were in their infancy, and though my hero attended one, most doctors were still trained by apprenticing themselves to doctors already in practice, and reading what textbooks were available. There was no national requirement that doctors attend a recognized medical school. Doctors saw patients in their office, but more patient visits took place when the doctor arrived in his black buggy.
When the story begins, Dr. Walker had just come out of the Civil War, in which he had been a doctor with the Union Army. In that war, as in many others, as many soldiers died of unsanitary conditions and contaminated food as died on the battlefield. Medical tents and buildings used for medical treatment were overcrowded and doctors worked around the clock, hampered by lack of supplies and knowledge. The most common treatment for wounds was amputation; the most common non-traumatic death was caused by dysentery.
Making Dr. Nolan Walker exceptional in his medical practice was more about what he didn’t use in the way of medical treatment than what he did. Many doctors of the time still used blood-letting as a treatment. One of the most popular medicines used was calomel, a compound whose main ingredient was mercury, which we know today to be a toxic substance. But back then it was used for almost every ailment, and was believed to be a stimulant, a cathartic (meaning it induced bowel movements) and an antimicrobial (though before bacteria were fully understood). Most often used for syphilis and given orally, it gave the patient foul breath, excessive salivation, and muscle trembling. It produced brain damage, and Dr. Walker was too smart to use it.
 |
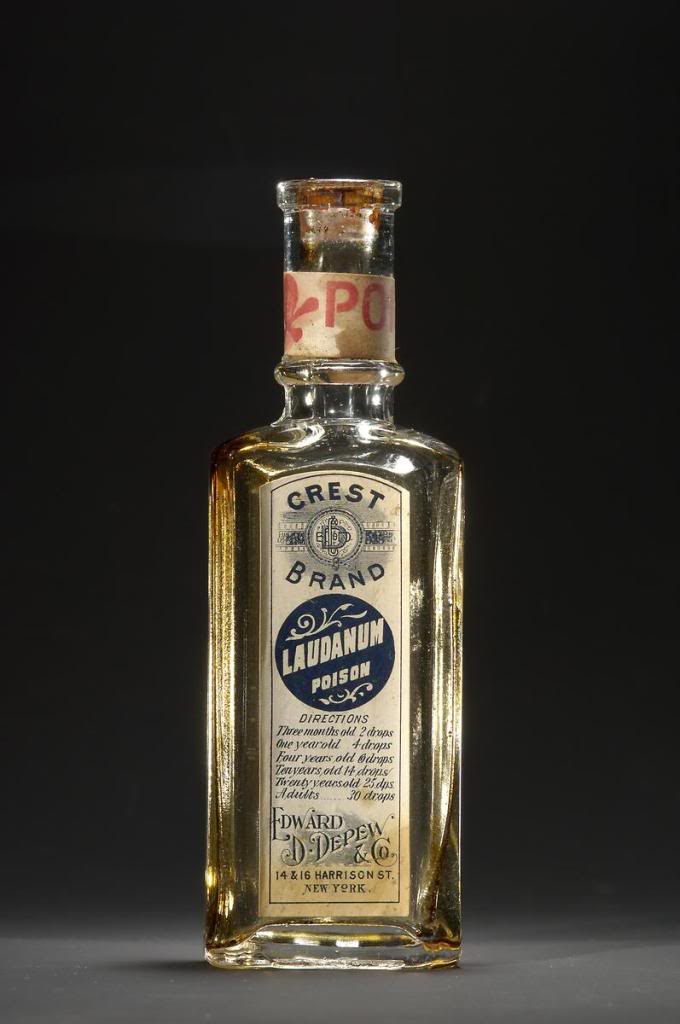
| AbSinthe_laudanum/PhotoBucket |
Another very common medicine was laudanum, and it was readily available over-the-counter. Its chief ingredients were opium and alcohol. Though useful as a sedative when that was truly needed, it was addictive and often abused. Even when used judiciously, it could produce nightmares in the patient.
The use of carbolic acid, discovered by Lister in Europe, as a disinfectant before and during surgery had just begun, but was not generally accepted. Many doctors still operated in street clothes and didn’t wash their hands between patients. Indeed, my doctor Walker was scorned as “fussy” by his fellow Army doctors for using it, but his amputation patients died much less often that those of his scorners. Dr. Walker uses it when Sarah Matthews falls and cuts her arm.
The wise doctors of the time, such as my hero, used remedies such as willowbark tea to reduce fever, and scorned the patent medicines sold over-the-counter and by medicine-show quacks. The key to treatment, in their view, was supportive therapy—any treatment which strengthened the body’s ability to heal itself. He believed in the tenet of the Hippocratic Oath which says “First, do no harm.”
It’s impossible to give a thorough summary of the state of medicine in the mid-1800’s in a blog. Indeed, it’s the subject of many fascinating and lengthy books. My object in this blog entry was to give you a quick glimpse of medicine as practiced by Dr. Nolan Walker in the town of Simpson Creek, Texas. (He appears in all my “Brides of Simpson Creek” books, including the one I’m writing now, when one of the main secondary characters suffers an apoplexy, or stroke.)
There were several books I used in writing THE DOCTOR TAKES A WIFE. Below is a list the ones I used most:
A Textbook of the Theory and Practice of Medicine, edited by Wm. Pepper, MD, W.B.
Saunders, 1893 (which I found in an antique store!)
A History of Medicine, Dr. Jenny Sutcliffe and Nancy Duin, Barnes and Noble Books,
1992.
Lotions, Potions and Deadly Elixirs: Frontier Medicine in America, Wayne Bethard,
Taylor Trade Publishing, 2004
Bleed, Blister and Purge: A History of Medicine on the American Frontier, Volney
Steele, MD, Mountain Press Publishing Company, 2005
Civil War Medicine, Robert Denney, Sterling Publishing Co., 1994
Thanks, Jordyn, for giving me this opportunity to talk about mid-1800’s doctoring and promote
The Doctor Takes a Wife and my other “Brides of Simpson Creek” books published by Love Inspired Historicals.
********************************************************************************
You can find out more about Laurie at her website: http://www.lauriekingery.com/index.html





 Today, I’m going to focus on a couple of general guidelines if you injure a character with some type of fracture.
Today, I’m going to focus on a couple of general guidelines if you injure a character with some type of fracture.