The one year anniversary of this blog was October 31st! Now that the zombies have been put to sleep for another year, it’s time to celebrate by taking a stroll down memory lane and looking at the top three most popular posts of the last year.
I love hosting Sarah Sundin. She’s a truly gifted novelist and I hope you’ll check out her books. This post, ranked #3, struck a chord with people and I think it’s the way Sarah painted the picture using her authorly ways to make this time period come alive.
In the 1940s, the local drug store was more than just a place to get prescriptions filled and pick up toothpaste—it was a gathering place. If you’re writing a novel set during World War II, it helps to have an understanding of this institution.
As a pharmacist, I found much about my profession has changed, but some things have not—a personal concern for patients, the difficult balance between health care and business, and the struggle to gain respect in the physician-dominated health care world. On February 14th, I discussed the role of the pharmacist in the 1940s, today I’ll describe the local drug store and how its role changed during the war, and on February 18th, I’ll review the rather shocking role—or lack thereof—of pharmacy and pharmacists in the US military.
Welcome to the Corner Drug Store—1939
Perkins’ Drugs stands on the corner of Main Street and Elm, where it’s stood all your life. Large glass windows boast ads for proprietary medications and candy, and a neon mortar-and-pestle blinks at you. When you open the door, bells jangle. The drug store is open seven days a week, sixteen hours a day, so you know it’ll always be there for you. To your right, old-timers and teenagers sit at the soda fountain on green vinyl stools, discussing politics and the high school football game. The soda jerk waves at you.
You pass clean shelves stocked full of proprietary medications, toiletries, cosmetics, hot water bottles, hair pins and curlers, stockings, cigarettes, candy, and bandages. You know where everything is—and if you can’t find it, Mr. Perkins or his staff will be sure to help you.
The owner, Mr. Perkins, is hard at work behind the prescription counter with good old Mr. Smith and Mr. Abernathy, that new young druggist Mr. Perkins hired last year. Mr. Perkins greets you by name, asks about your family, and takes your prescription. He has to mix an elixir for you. If you don’t want to wait, he’ll be happy to have his delivery boy bring it to your house. But you don’t mind waiting. You have a few items to purchase, and you’d love to sit down with a cherry Coke.
Welcome to the Corner Drug Store—1943
Perkins’ Drugs still stands at the corner of Main Street and Elm. Large glass windows boast Army and Navy recruitment posters and remind you that “Loose Lips Sink Ships.” The neon sign has been removed to meet blackout regulations. The store is open for fewer hours since Mr. Smith retired and Mr. Abernathy got drafted. Mr. Perkins hired Miss Freeman. Not many people are thrilled to have a “girl pharmacist,” but if Mr. Perkins trusts her, that’s good enough for you. Perkins’ Drugs and Quality Drugs on the other side of town alternate evening hours so the town’s needs are met.
A placard on the door reminds you that Perkins’ Drugs is authorized by the Office of Civilian Defense as a pharmaceutical unit, meaning the store will provide a kit of medications and supplies for the casualty station in case of enemy attack. You pray the town will never need it.
Bells jangle when you open the door. The soda fountain is closed. Mr. Perkins can’t buy metal replacement parts for the machine, the soda jerk is flying fighter planes over Germany, and sugar is too scarce a commodity.
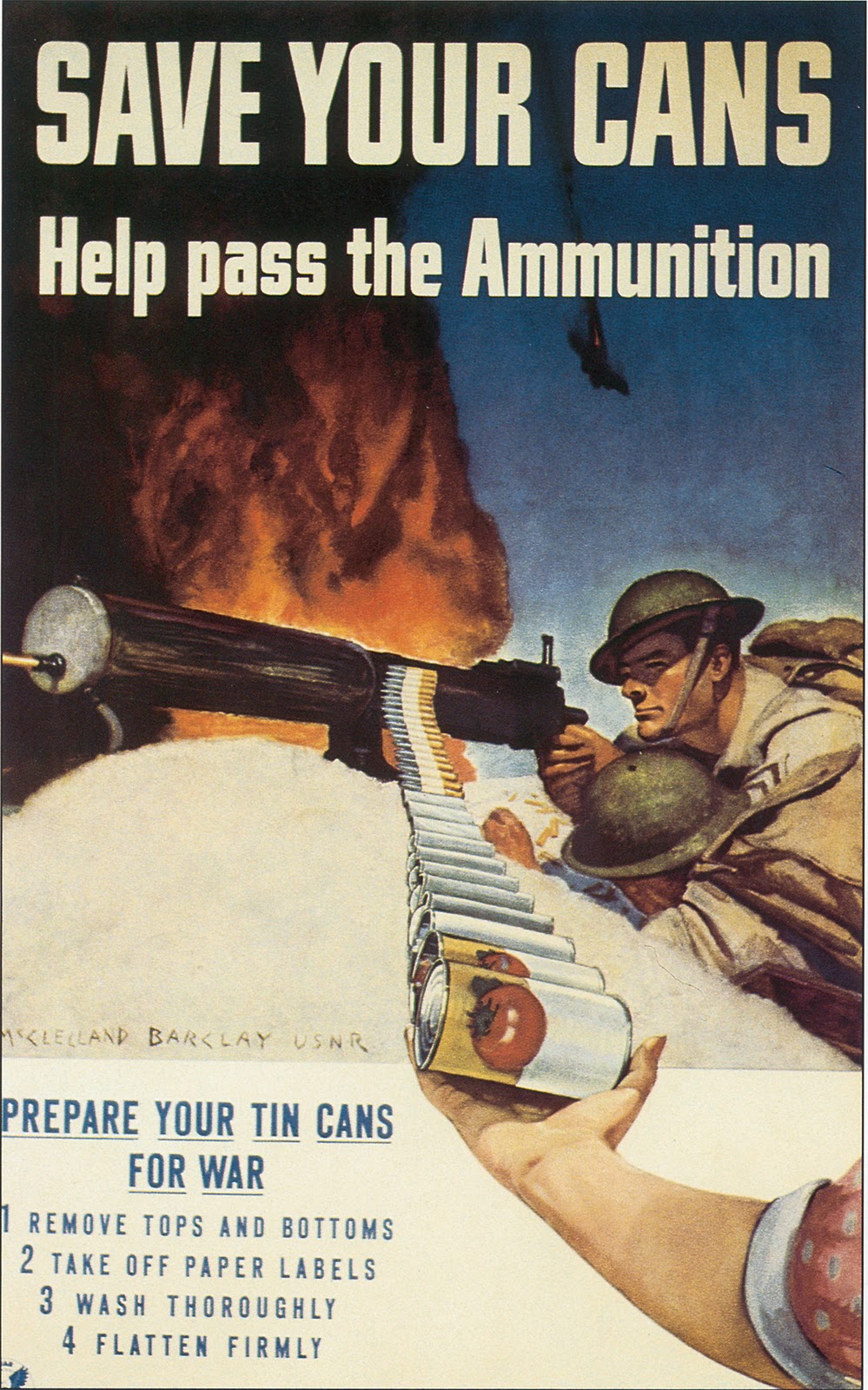
A barrel stands by the door. You toss in five tin cans, washed, labels removed, tops and bottoms cut off, and flattened. Mrs. Perkins at the cash register thanks you.
You pass clean shelves with depleted stocks. Proprietary medications, cosmetics, toiletries, and medical supplies remain, but rubber hot water bottles, silk and nylon stockings, hair pins and curlers, candy, and cigarettes are in short stock—or unavailable. Most of the packaging has changed. Metal tins have been replaced by glass jars and cardboard boxes. You pick up a bottle of aspirin and a tube of toothpaste, double-checking that you brought your empty tube. Without that crumpled piece of tin, you couldn’t purchase a replacement. Tin is too dear.
At the prescription counter, Mr. Perkins greets you by name and asks about your family. Miss Freeman gives you a shy smile and you smile back. There’s a war on and women have a patriotic duty to do men’s work so men are free to fight. Mr. Perkins frowns at your prescription for an elixir. He’s used up his weekly quota of sugar, and his stock of alcohol and glycerin are running low. Would you mind capsules instead? Of course not. Mr. Perkins phones Dr. Weber and convinces him to change the prescription. Mr. Perkins can’t have the prescription delivered—he doesn’t qualify for extra gasoline and he couldn’t find a delivery boy to hire anyway.
You and Mr. Perkins discuss war news as he sets up a wooden block with little holes punched in it, then lines the pockets with empty capsule halves. He weighs powders on a scale, mixes them in a mortar, then fills the capsule shells. After he sets the capsule tops in place, he puts the capsules in an amber glass bottle with the familiar Perkins’ Drugs label.
You buy a few War Bonds. Your wages are higher than ever with the war on, and with all the shortages there’s nothing to buy. Besides, War Bonds are a solid financial investment and your patriotic duty. On a poster by the counter, a smiling pilot leans out of his plane and reminds you: “You buy ‘em. We’ll fly ‘em. Defense Bonds and Stamps.”
Mr. Perkins thanks you for your purchase, and you thank him for his service. War or no war, you know Perkins’ Drugs will always be there for you.
Resources
My main source was this excellent, comprehensive, and well-researched book: Worthen, Dennis B. Pharmacy in World War II. New York: Pharmaceutical Products Press, 2004.
http://www.lloydlibrary.org (Website of the Lloyd Library and Museum, which has many articles and resources on the history of pharmacy).
*****************************************************************
Sarah Sundin is the author of the Wings of Glory series from Revell: A Distant Melody (March 2010), A Memory Between Us (September 2010), and Blue Skies Tomorrow (August 2011). She has a doctorate in pharmacy from UC San Francisco and works on-call as a hospital pharmacist