When my debut medical thriller, Proof, was going through the editorial process there was a question about a particular character’s reaction to finding his friend, and love interest, attacked and unresponsive in her home.
Kadin Daughtry is an OB/GYN. So, he’s used to being under pressure. After all, babies can be in a rush sometimes to be born.
 However, when he finds Lilly, beaten, he does the necessary things– checks her pulse, calls 911. But he is stunned and having difficulty.
However, when he finds Lilly, beaten, he does the necessary things– checks her pulse, calls 911. But he is stunned and having difficulty.
Editorial thought he should have his act much more together– after all, he is a trained physician.
Hmmm….
It’s true, medical people have the knowledge to deal with emergencies. But they still are people and can suffer the same reactions other people under stress will feel.
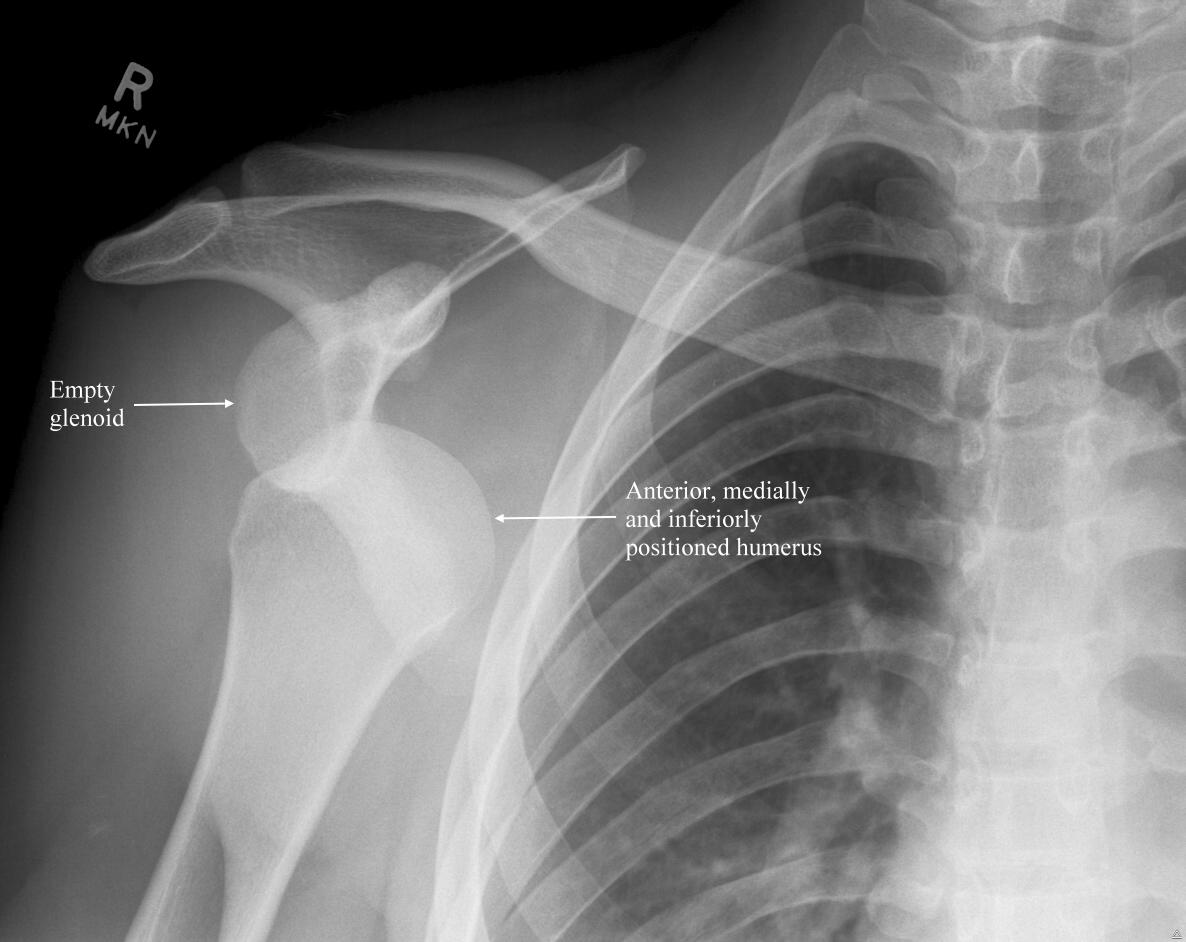
About nine months ago, I dislocated my shoulder while working out with a personal trainer. Unfortunately, this was not a new thing (to the left shoulder it was!) so, initially, I felt like– okay, I can manage this. We just need to get it back into place as I’d been able to self reduce my right shoulder before.
The pain was pretty awful. No quite as bad as burning my eyeball with a curling iron (yes, the actual eye!– I know– it takes talent) or giving birth but up there. When it became clear that I wasn’t going to be able to reduce it myself and wasn’t willing to let my trainer try because he doesn’t carry Fentanyl in his pocket– in retrospect I realized a couple of things.
1. Pain makes it really hard to think. It doesn’t matter how well versed you are about treatment of certain injuries, pain makes it hard to think through your options. You just want the pain to stop– quickly.
2. Because of #1– making decisions is hard. It’s not that your clinical brain checks out. You can still assess the injury and walk someone else through the treatment, but it’s not seemless. Meaning, there were long moments of silence as people waited for me to tell them what to do because they know I’m an ER nurse.
3. You really want someone else to make the decisions. Even though I am an ER nurse, I really wanted someone else to step up and say– this is what I’m going to do and this is what I need you to do. We’re going to get you up. I’m going to call an ambulance… It’s reassuring to feel that someone has your back. When people are doubtful around you and looking horrified at your injury– you begin to worry about yourself more. That’s why having that “doctor face” is important. People want to feel like you can competently handle whatever is wrong with them.
4. Ambulance rides are very bumpy! Don’t ever write that an ambulance is a comfortable ride. They are not.
What about you? Have there been times people looked to you to be an expert but you really needed someone else to step in?