Sometimes television dramas get it wrong. And then there are times they miss the mark so spectacularly you wonder if they had a consultant on set or just decided on a quick Google search to not slow production down. The Rookie Season 4, Episode 17 (“Coding”) firmly plants itself in the latter category.
A young woman is injured in a motor vehicle collision, dies, and is declared dead on scene from a devastating abdominal injury. Nolan is asked by his firefighter girlfriend, Bailey, to check her driver’s license to see if she’s an organ donor. Check and check. Next cut is her arriving to the hospital with an honor walk already waiting and she’s taken directly to the OR for donation. The only problem? Medicine doesn’t quite work that way. Or at all.
The patient is shown being intubated (so far, so good), but the team isn’t performing compressions. Small problem– she has no pulse. For organs to be viable, blood needs to circulate. Without CPR maintaining blood flow, those organs are not viable for transplant.
In TV land, organ donation is apparently as easy as checking a box on your driver’s license. In reality, donors undergo extensive testing—blood typing, infectious disease screening, toxicology, and so much more. It’s a lengthy, arduous process.
Yes, it’s television. Yes, we suspend disbelief. But medical inaccuracies like this reinforce misconceptions about organ donation. Families already face difficult decisions during an impossibly hard time. Feeding audiences the idea that hospitals snatch organs from people who just happen to check the donor box doesn’t do much to build trust in the system.
The ironic part? Organ donation stories can be powerful, emotional, and medically accurate. Real life has plenty of drama without rewriting basic physiology. You don’t need to sacrifice science to tell a compelling story.
Ah, Dexter. Few shows juggle serial killing, dark humor, and wildly inaccurate hospital scenes quite like you. In Season 4, Episode 2, our favorite blood-spatter analyst wrecks his van—with a dead body conveniently riding shotgun in the back—and winds up in the ER. What follows is a crash course in how not to portray medicine on television.
Let’s dissect, shall we? (Pun very much intended.)
The ER doctor shines a light into Dexter’s eyes. Normal practice? Sure. But then we’re treated to the statement that his pupils dilate. Pupils constrict when you shine a light into them. They dilate in darkness. This is how the human body properly works.
Next, the doctor looks at Dexter’s CT scan and announces, “You’ve sustained a concussion.” implying that concussions are diagnosed this way. Concussions can be clinically diagnosed, based on symptoms like headache, confusion, dizziness, and loss of consciousness. You don’t need a CT scan to tell you that, and a CT isn’t going to show a concussion anyway. If it does, congratulations—you’re likely now dealing with a bleed, not a simple concussion.
But hey, why rely on pesky medical standards when you can dramatically gesture at a glowing scan instead?
Then comes one of my favorite relics of outdated medical lore: the “Don’t let him sleep” after head injury rule. Dexter is told not to sleep for twelve hours, as if a good nap might somehow erase him from existence.
In reality? We don’t keep people awake anymore after they’ve suffered a head injury if they feel like they need to sleep. That advice has gone the way of lobotomies. Any injured body part needs rest to heal. The brain rests by sleeping. Sleep is good and beneficial for the head injured patient. The guidance is: let the patient rest, check in periodically if symptoms worsen, and maybe—just maybe—don’t torture the poor guy who just got his bell rung trying to hide his crimes.
Ultimate lesson– don’t get into a car accident with a body in the back of your van that the police are going to tow.
Which show do you think butchers medical accuracy the most and which on gets it right?
In the Season Two/Episode Eight airing of the FOX television show 911— there was a great scene on how to really provide no medical care.
The setup: A gay couple is getting ready to go on a bike ride. Much time is spent in a musical montage showing their lives together. It’s clear they have had a loving relationship and remain deeply in love. One gentlemen goes to load a bike onto a SUV when, in a series of unfortunate events, he gets pinned by the SUV to the entrance gate— akin to Anton Yelchin’s accident (though they do show in the episode the SUV was placed in neutral).
He is discovered by his partner who then calls 911. Upon arrival, there isn’t much done for his lover. He is essentially declared dead on arrival.
Then, the gentleman who discovered his partner, goes unconscious while a firefighter has his back turned. Literally only a few seconds have expired when the firefighter discovers he’s passed out. They provide one and a half cycles of CPR and kind of shrug their shoulders declaring that he’s died, too.
This is unacceptable management of this patient. It’s essentially a witnessed arrest so they were correct to start CPR immediately, but at the very least, he should have been connected to an AED for rhythm analysis and probable defibrillation. A very common reason for sudden collapse are arrhythmias that will respond to electricity. There’s no reason why this gentleman’s treatment should have been so sparse. It would have increased the drama and the tension of the episode to have this patient get a full resuscitation.
In a book I am working on the main character falls off of a one-story wall injuring his back. Could he be paralyzed? If so, would it be possible for paralysis to set in an hour or two later? Would he be able to remain conscious and still walk for about an hour? He is a spy, mid 20’s, strong, and loves to run.
Jordyn Says:
In my experience, I’ve never seen a delay in onset of paralysis. Usually, it is immediate. I’ve not personally seen people with devastating paralysis from a fall from this height. Broken legs/arms, lacerations, and concussions . . . sure. Could a spinal cord injury happen? Of course there are always outliers. If you did write this, it would help believability if the character fell directly onto their head (called an axial loading injury) or onto another hard object (like a rock or something with a hard edge) to increase the chance of a complex fracture causing paralysis.
I did some hunting regarding spinal bones specifically. This article says three meters (which equates to about 10 feet or one story) can cause spinal fracture, but just because you break the bones doesn’t necessarily mean paralysis. A person with a stable fracture of their back can be up and walking around. I’ve seen this plenty of times.
I did find one article where a woman did have delayed onset of paralysis of four days, but if you read through the article she had a significant mechanism of injury and died as a result of complications of her injuries.
Hi there! I’m so glad I’ve found your site and thanks for taking the time to read this. Ok, here goes.
I’m writing about a fifteen-year-old boy who is being abused physically and sexually by his father. One day at school, he tries to commit suicide by slitting his wrists. He becomes scared by the amount of blood, so he leaves the restroom to try to find help. He is found by his teacher and passes out. Now, I know with any kind of suicide attempt, the police are always contacted, and given the all clear for the paramedics.
Jordyn: I think it would depend on the city, county, school district (and whether or not there was a school resource officer) as to the level of police involvement if he just really needs medical attention. I would advise that if this is written about a real place you ensure they have co police response because a paramedic team would be able to handle this call.
Pink: What will the ED staff do to stabilize a patient who has slit their wrists? Is surgery necessary if the wound is pretty deep?
Jordyn: We always look at airway, breathing, and circulation first. If the patient is talking to us then we can quickly check off the first two as at least functional for the time being. As far as circulation the priority is to stop all active bleeding first by direct pressure. Also, does the patient exhibit any vital sign measurements that show he’s suffering from blood loss—which in this case could be increased heart rate, low blood pressure, and also low oxygen levels.
After that, the medical priority for this patient is to further control the bleeding and determine how much blood he’s already lost. Direct pressure is the method used to control the bleeding. Blood work would be done to look at his blood counts to see if he needs any blood replacement. Next would be to look at if he damaged any arteries, tendons, ligaments or nerves during the attempt. Generally, an exam of the function of the fingers can reveal if there is a concern there. For instance, do his fingers have full range of motion? Do any fingers have areas of numbness? Arterial bleeding is very distinct so it’s usually obvious if an artery has been severed. If he has damaged anything that would limit the function of his hand then he would need follow-up evaluation by a hand surgeon for surgery. If there is no damage to the structures as listed, there is a possibility the wound could be closed in the ER as a simple laceration repair.
Pink: Upon discharge, what will the patient be given to take home for treatment of their wound (the slit wrist)?
Jordyn: If the patient gets a simple laceration repair (merely closing the skin even if it takes a lot of stitches) then pain could be managed at home with over-the-counter pain relievers like Tylenol or ibuprofen. If the patient requires surgery, a short course of a narcotic may be given for pain control, but we also have to look at other factors to determine if this would be wise for the patient (are they a current drug addict or is there continued concern for suicide attempt). If the patient has surgery, then it is up to the surgeon to determine the patient’s home pain relief.
Pink: If a nurse or doctor notices any bruises on the patient’s body, can they examine an unconscious patient?
Jordyn: Yes, an unconscious patient’s skin can be externally examined. In fact, it is often protocol to do so because we are looking for clues as to why the person is unconscious.
Flatliners 2.0 released in October, 2017. If you haven’t seen the movie (or the original from 1990) then you may not want to read this post as there will be spoilers involved.
Flatliners centers around a group of medical students who become curious with the phenomenon of near death experiences (NDEs) to the point that they “flatline” one another so that they can purposefully have one.
This first post will deal with a medical scenario that happens in the first ten minutes of the film. We’ll look at two screenshots from the movie.
Here is the conversation among the medical students when their new patient arrives.
Paramedic: “Transfer from Holy Cross. Thirty-eight year old construction worker fell off a beam. Persistent coma. GCS 6.”
Marlo: “Standard procedure for a GCS 6 admit calls for 2 large bore IVs and diazepam on standby.”
Ray: “Seizure meds won’t do any good. Whatever is wrong is in his spinal column and not in his brain.”
Marlo: “And what medical protocol are you citing?”
Ray: “The protocol of actually living in the real world. Where guys with crappy HMO’s go undiagnosed with spinal injuries.”
Marlo: “Actually he’s on seizure meds which is a medical protocol of reading his chart.”
At this point an alarm sounds and the students begin to panic. This is the screen shot at the moment of panic. It shows the monitor. The patient’s heart rate is a nice steady 73. His oxygen level is 100%– can’t get any better than that. His respiratory rate is 19– the patient is on a ventilator. I don’t know– things looks pretty good to me for this patient.
An attending doctor arrives.
Attending: “What is it?”
Student: “Respiratory failure.” (Based on the screen shot, there is no basis for this. Also, nothing is quite hooked up correctly at the head of the bed for an ER.)
Attending: “He might be hemorrhaging. Page neurosurgery, call a code, and get CT on standby. Students, clear the room!”
They then show another monitor in the room which appears to show ventricular fibrillation (V-fib) which is a lethal, but shockable rhythm. Yet, no one starts CPR.
End Scene.
Issue #1: I’m not sure how a medical student within the first ten seconds of getting this patient can know if the problem is in the brain or the spinal cord. For me, the problem seems likely to BE in the brain considering his persistent vegetative state.
Issue #2: Because of the patient’s insurance, he didn’t receive an accurate diagnosis. Mmmm . . . I know this myth get’s perpetuated. You don’t necessarily need expensive tests ALL the time to get an accurate diagnosis. CT scans and MRI scans aren’t really seen as extreme measures anymore. Though they are expensive the cost has come down.
Issue #3: Nothing these medical people say makes any sense medically. What evidence is there that the patient is in respiratory failure? The photo of the first monitor doesn’t suggest that. What evidence is there that the patient is hemorrhaging into his brain? Fixed and dilated pupils? Unequal pupils? A worsening coma score? None of that is presented in the scene.
Issue #4: The one medical problem they seemingly show is the V-fib in the second screen shot. Good to call a code, but research has shown that early and effective CPR is the one thing that is best at bringing people back. The next is early defibrillation which no one seems to anxious to accomplish.
Is it that hard to find good medical consultants for movies?
This television episode caused more people to reach out to me over any other. This Is Ushas been building up to Jack’s death for eighteen months. It needed to be big. It needed to be dramatic. Can you tell I’ve been watching the show? It was really none of those and medically— well, just weird to be honest.
If you haven’t watched the episode then don’t read this post because it will reveal his cause of death . . . like right now.
Jack’s ultimate demise? A heart attack called the widow maker caused by the stress of the fire.
Jack is in intense smoke and heat for several minutes. He emerges and is first checked by EMS. He is being given oxygen and a dressing to his arm for “2nd degree burns”. The EMS person says she can’t treat the burn and he is seemingly refusing transport, but she does encourage him to be seen. Also, giving oxygen is correct, but it is not the right type of mask. A note on burns. Burns will evolve over the next several days so you don’t really know how severe a burn will be for a while.
Jack does eventually go to the hospital to get his burns checked. The doctor is initially giving him instructions on burn care. The doctor says, “I’d like your heart rate to come down.” and glances at the monitor— which doesn’t have any readings on it. No waveforms. No numbers. He then says, “There’s soot in your airway so we’ll have to run some tests. The swelling is minor.”
That’s about it. The doctor tells Jack he basically dodged a bullet and seems none too concerned about his potential airway damage.
Just as I mentioned above, airway burns from smoke inhalation are similar to skin burns in that they evolve over time. Smoke inhalation and the potential for upper airway swelling is taken very seriously. There is a nice overview here. At the very least, there should be discussion of admitting Jack to the hospital. As quoted from the article, “Studies have shown that initial evaluation is not a good predictor of the airway obstruction that may ensue later secondary to rapidly progressing edema.” If there is concern about significant injury to the airway then the patient is electively intubated until the airway injury heals. It’s VERY difficult to intubate someone with a lot of airway swelling.
Shortly after this consultation, Rebecca decides to make a phone call and get a candy bar from the vending machine. In that, perhaps under two-three minutes passage of time, Jack codes and dies. Even though she is just outside the ER nurses station, she never hears a code being called. Doesn’t see the commotion.
The doctor approaches her and says, “One of complications of smoke inhalation is that it puts a terrible stress on the lungs and therefore the heart. Your husband went into cardiac arrest. It was catastrophic and I’m afraid we lost him . . . Mrs. Pearson, your husband has died.”
After a few exchanges she goes to Jack’s room where there is a spotlight shining on his chest with a cursory ambu bag at the head of his bead . . . but no other equipment. I’m telling you in two minutes, a code has barely just begun and is never called so hastily . . . like ever. Later, explaining the event to Miguel, Rebecca says he had a widow maker’s heart attack.
There would be no realistic way the doctors would know it was specifically this kind of heart attack as shown in the episode without an autopsy. Presumably, Jack went into one of the lethal heart rhythms, v-tach or v-fib, at the time of his code. In the time frame given on the show, the medical team would have barely started CPR and given the first line treatment which is electricity. A 12-lead ECG can be a strong diagnostic tool for this type of heart attack, but they never did one. Had they done that early on, they probably would have seen the changes.
Also, he would likely have some signs and symptoms. Chest pain. Nausea. Left arm pain. Sweating. Demonstrating these might make the scenario seem more believable. Having Rebecca witness the code would have been more dramatic.
Also, it would make more sense that he would suffer this cardiac event while he is actually under duress— such as during the rescue of the children and the dog.
The only way to truly know that this is the type of heart attack Jack suffered as presented in the show would be to conduct an autopsy.
This Is Us— thanks for killing off a beloved character in a totally lame way— at least from a medical standpoint.
In Episode 3 of 9-1-1, the story opens with officer Athena Grant, played by Angela Bassett, finding her daughter unconscious from taking hydrocodone pills as seen in the trailer below. The daughter, who appears to be between twelve and fourteen, is whisked off to the hospital and admitted to the ICU in short order. One, did they treat this ingestion (or overdose) correctly? Two, would this type of ingestion warrant ICU admission?
It’s stated in the episode that the daughter took “six to seven” hydrocodone pills. Hydrocodone is a combination of acetaminophen (Tylenol) and a synthetic type of codeine. It comes in many different preparations with different amounts of acetaminophen and hydrocodone. Where do we start to evaluate whether or not the ingestion is worrisome?
1. How is the patient? What signs and symptoms do they have? The EMS crew in this situation is lucky. The mother knows exactly what the daughter took. She presents unresponsive with slow breathing. Number one treatment in this situation after assisting with her breathing? Give Narcan which this crew absolutely does not do. Narcan is a reversal agent for opioids. It can be given via a mist up the nose so you can generally reverse the sedative effects of the drug without even starting an IV. It is a life saving measure because it is the not breathing part that will kill you first. This is the medication they should have given first.
2. What did the patient take? When did they take it? How much did they take? Many drugs have multiple components and we have to evaluate EACH component and whether or not this could prove harmful to the patient. The opioid (once reversed with Narcan) is probably the least concerning. The amount of acetaminophen ingested is our next priority and we would calculate how many milligrams per kilogram she took. We know for acetaminophen that when you start to get between 100-150mg/kg that there could be a potential for liver damage. There is a reversal drug for acetaminophen’s damaging effects on the liver called Mucomyst, but there is a window in which this can be given to be effective. Usually, a poison control center will help us manage these types of patients.
In this case, let’s say she took six pills of Lortab 7.5/500. From this we know that each pill has 500mg of acetaminophen. Assuming the average 12-14 y/o is about 100 lbs (converted to 45 kg) then she took about 66mg/kg of acetaminophen. A four hour Tylenol level (measured four hours after the ingestion) would be checked to ensure she wasn’t toxic, but in this case likely not.
3. Will this patient be admitted to the ICU? It might come as a surprise, but ingestions of medications are most often not admitted to the ICU. Most are managed and observed in the ER. In this case, the girl should have been given Narcan by EMS. We would continue to watch for the somnolent effects of the opioid and evaluate the risk of the acetaminophen.
Also, it’s generally protocol that an aspirin level is measured as well even if the patient denies taking any. We can’t always depend on the patient being truthful about what they took and aspirin can have very devastating effects as well. Other labs depend on the medication ingested and what parts of the body if affects. This patient would likely not be admitted to the ICU.
Also, if we get a toxic ingestion within an hour we can give activated charcoal (that literally looks like black sludge) that will bind the medication. This is not always done for several reasons. One is the risk of the charcoal ending up in a patient’s lungs during administration. Usually this is done under the recommendation of Poison Control.
4. Do we notify Child Protective Services? In this episode, Child Protective Services conducts a mental health exam on the teen. In the real world, this evaluation takes place through mental health providers not associated with the state. State involvement is generally reserved for what we would consider a risky home environment. A teen getting into their parents medicine cabinet for some pills would not fall into that category. What would? A two-year-old ingesting crack cocaine that was lying around the home. Each case is handled very individually, but this case presented in 9-1-1 would not rise to that level in my opinion.
As a side note, parents are not separated from their children during medical treatment. Can we please stop perpetuating this myth?
I’m so happy to be back blogging! I hope everyone had a fantastic holiday season and is ready for a new year. Today is officially my 20th wedding anniversary! Can you believe that? I know I can’t. It’s crazy to think how much time has gone by.
Considering the occasion, I thought it would be best to write a positive (well, mostly positive) review of a new TV show— Fox’s series 9-1-1. I know . . . you can pop your eyeballs back in. This is truly a rare event considering much of this blog’s time is spent skewering medical inaccuracies in print, movies, and the small screen.
9-1-1 is a series devoted to dispatch, police, and fire calls. I’ve watched the first two episodes and was pleasantly surprised at how much I liked it. Now, it does have some problems. Writing completely to stereotype would be the biggest.
Let’s look at what they did well.
1. The characters face consequences for their actions. I’ve said all along that it’s okay for medical people to do bad things in fiction, but there must also be consequences for their actions. The point of this are many. It increases the conflict in the story AND reflects real life. Too many times in fiction medical people are shown doing bad things without consequence. One firefighter is shown facing some serious repercussions for his poor (saying that lightly) choices.
2. There is respect for HIPAA and also how hard that is for medical people. HIPAA is the patient privacy law. Because of HIPAA, most of us who work on the front lines (EMS and emergency departments) rarely ever hear how our patients do after they leave our care. This is, flat out, not easy for any of us and it makes closure difficult.
3. Shows the problem of poor coping mechanisms. It is true that healthcare people do not always have the best coping mechanisms. Hello, to all the nursing units with the mandatory chocolate drawer. Some develop addictions and can have bad co-dependent relationships. It was nice to see highlighted that the stress of this work does take an emotional toll.
4. Highlights the difficulty of work/life balance. Of course, all professionals face work/life balance issues, but I also feel like the nature of our work makes it hard to feel like you’re getting a break. If you’re taking care of a medically/terminally ill loved one at home, and then go to work doing the same thing— there can be little room to breathe.
5. Medical information was not distracting. The medical information was kept pretty light in the first two episodes and not too distracting. There were a few minor medical errors I’ll keep close to the vest for now.
Have you watched the new Fox show 9-1-1. What did you think?
Nothing probably tugs at the heartstrings more than thinking about a child dying. It’s not the way things are supposed to happen. We expect life to follow the natural order of things— the old die first. Parents should never bury their children.
Sadly, we know this reality is not true. The pediatric nurse understands and confronts this reality more often than most. Particularly nurses who work critical care, ER, oncology, and hospice.
A reader of this blog posed this question to me: How long will a nurse or doctor perform chest compressions on a pediatric patient? Is forty-five minutes too long or would they try longer?
This is a tough question and not so easily answered. There are really no hard and fast rules as to when CPR should be stopped and it depends a lot on the reason for the code (if known) and what types of signs the patient is giving us. For instance, just because a patient doesn’t have a pulse, doesn’t mean they don’t have electrical activity in the heart muscle. Some causes of a code are reversible, but it takes time to do so. Hypothermia might be a good example of this.
I’ve worked in both adult and pediatric critical care. What I’ve found generally is providers will run pediatric codes longer than adult codes even when chances are small to get a pulse back. No one wants to see a kid die— health care providers are no different. Plus, culturally, we resist death at every turn even though it is the course each of us will journey to.
1. Are there clinical features present prior to the code that are predictive of poor survival? For instance, in the adult patient some of these from the article included pneumonia, metastatic cancer, and low blood pressure. For pediatric patients, kidney failure and use of a continuous infusion of epinephrine are mentioned.
In the emergency department setting, we want to know what the patient’s initial heart rhythm was. If there was no electrical activity in the heart (terms such as asystole, flat-line, ventricular standstill) then chances of getting back organized electrical activity AND contraction of the heart muscle are low.
2. Is the patient receiving high quality CPR? This might seem like a no brainer. Of course, if the patient codes in the hospital, they must be receiving excellent CPR. What research shows is that this is not true and it is a big drive of many institutions to simply improve the quality of CPR. If I can ease your mind, many hospitals are improving CPR basics through high fidelity code labs, more frequent CPR check-offs, mock codes, and computer based CPR training that measures effectiveness of CPR and coaches the participant on how to improve .
What are some CPR pitfalls? Initiating CPR in a timely manner. Compressing deep enough and at the right rate. Not over or under ventilating the patient (both can actually cause problems). CPR is what we call a high risk, low yield procedure— meaning we don’t do it very often, but when we do we have to do it right. What you don’t practice frequently you don’t become adept at. CPR is no different.
Considering this, we look at how long the patient’s down time was. This refers to the time when the patient’s heart stopped beating to the time they got CPR. Trouble is, this might be relatively hard to determine. When was the patient last seen? Is the patient cold to the touch? Are their pupils fixed and dilated?
The good news for the writer is there is a lot of leeway in this area as far as how long a medical team might “work” on a patient. Factors can be given for both short and long resuscitation times.
The most important part is getting those factors medically correct.
What about you? Have you written a resuscitation scene into a work of fiction?

 The setup
The setup In a book I am working on the main character falls off of a one-story wall injuring his back. Could he be paralyzed? If so, would it be possible for paralysis to set in an hour or two later? Would he be able to remain conscious and still walk for about an hour? He is a spy, mid 20’s, strong, and loves to run.
In a book I am working on the main character falls off of a one-story wall injuring his back. Could he be paralyzed? If so, would it be possible for paralysis to set in an hour or two later? Would he be able to remain conscious and still walk for about an hour? He is a spy, mid 20’s, strong, and loves to run. I’m writing about a fifteen-year-old boy who is being abused physically and sexually by his father. One day at school, he tries to commit suicide by slitting his wrists. He becomes scared by the amount of blood, so he leaves the restroom to try to find help. He is found by his teacher and passes out. Now, I know with any kind of suicide attempt, the police are always contacted, and given the all clear for the paramedics.
I’m writing about a fifteen-year-old boy who is being abused physically and sexually by his father. One day at school, he tries to commit suicide by slitting his wrists. He becomes scared by the amount of blood, so he leaves the restroom to try to find help. He is found by his teacher and passes out. Now, I know with any kind of suicide attempt, the police are always contacted, and given the all clear for the paramedics. Flatliners centers around a group of medical students who become curious with the phenomenon of near death experiences (NDEs) to the point that they “flatline” one another so that they can purposefully have one.
Flatliners centers around a group of medical students who become curious with the phenomenon of near death experiences (NDEs) to the point that they “flatline” one another so that they can purposefully have one.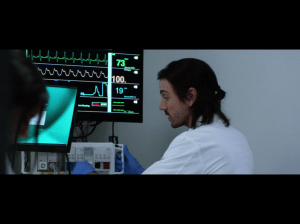 Ray: “The protocol of actually living in the real world. Where guys with crappy HMO’s go undiagnosed with spinal injuries.”
Ray: “The protocol of actually living in the real world. Where guys with crappy HMO’s go undiagnosed with spinal injuries.” Attending: “What is it?”
Attending: “What is it?” The widow maker is a real term for a heart attack.
The widow maker is a real term for a heart attack.  Considering the occasion, I thought it would be best to write a positive (well, mostly positive) review of a new TV show— Fox’s series
Considering the occasion, I thought it would be best to write a positive (well, mostly positive) review of a new TV show— Fox’s series  Sadly, we know this reality is not true. The pediatric nurse understands and confronts this reality more often than most. Particularly nurses who work critical care, ER, oncology, and hospice.
Sadly, we know this reality is not true. The pediatric nurse understands and confronts this reality more often than most. Particularly nurses who work critical care, ER, oncology, and hospice.