For a long time, I was an avid medical show consumer– whether it be reality or scripted. The reality based ones, that highlight functioning ER’s, are tolerable. The scripted ones just started to drive me crazy and I haven’t partaken in a medical fiction series in a while. I’ll let you know about my trauma related to watching Rescue: HI-Surg in another post(and I’m not even a lifeguard).
Unfortunately, that doesn’t stop other shows from violating medical accuracy. Why does accuracy matter? It proves to the consumer of the product that you took care to present something close to reality. Our goal should also be to keep them in the story bubble. Any time a reader is pulled out of that magic snow globe, they lose pace and connection with the story.

Which brings me to Netflix’s The Perfect Couple. The basic plot is a woman from a modest background marrying into high society when her best friend, and maid of honor, shows up dead on the beach. The series delves into all the ins and out of who murdered her.
At one point, they show the victim’s toxicology report and I’m including a screen shot of said evidence.
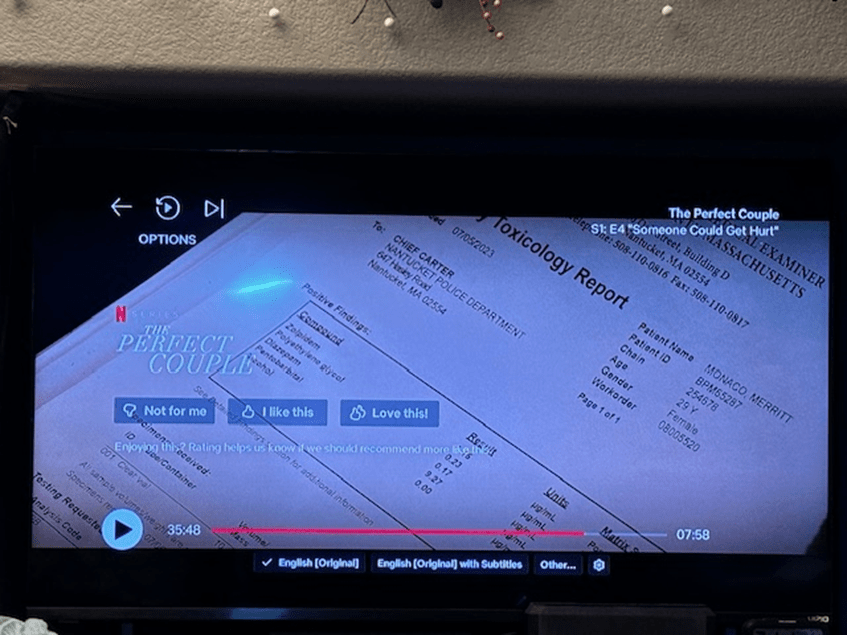
This is hard to read so I’ll give you the details. In the victim’s urine (presumably– the report doesn’t specify) are the following drugs:
1. Zolpidem (Ambien)– sleep agent
2. Polyethylene Glycol– (Miralax)– laxative
3. Diazepam (Valium)
4. Pentobarbital (Barbiturate) Central Nervous System Depressant
5. Alcohol
This report confused me. Why would a dramatic television show reveal the victim was positive for a laxative? Which, by the way, isn’t going to show up on a drug screen.
Then it hit me. My belief is the writing staff really meant this fictitious toxicology report to read “ethylene glycol” which is very different. Ethylene glycol is a highly toxic component typically found in antifreeze. Antifreeze tastes sweet, which is why pediatric patients will continue to drink it if they find it in an open container. It has disastrous effects on the body and can cause death quickly if proper medical treatment isn’t enacted (and even then– it’s dicey).
This toxin also isn’t going to show up on a standard drug screen. The medical team is going to have to look for it specifically and such a niche test isn’t going to be available at every medical center. Also, Ambien is not part of a baseline drug screen.
Wouldn’t it have been more interesting to the plot to have antifreeze found in her system?
What strange things have you noticed on medical show toxicology reports?
 I’m hoping for any input you have at least in the abstract. For instance, would you give the patient more concentrated doses, more frequent doses, larger doses? What kind of medicines would be prescribed/would correlate with the metabolism bit in context of painkillers and treatment of a gunshot wound?
I’m hoping for any input you have at least in the abstract. For instance, would you give the patient more concentrated doses, more frequent doses, larger doses? What kind of medicines would be prescribed/would correlate with the metabolism bit in context of painkillers and treatment of a gunshot wound? The second episode sees Shaun begin his duties and he’s been accepted into the program, albeit with some outward disdain from some of the attending surgeons.
The second episode sees Shaun begin his duties and he’s been accepted into the program, albeit with some outward disdain from some of the attending surgeons.