Carol Asks:
I’m writing a scene that involves a child approximately eighteen-months-old. She was submerged for an unknown period of time (no more than a couple of minutes) on a beach after being struck by a rogue wave that knocked her down.
 When found, she has a pulse, but is not breathing. Rescue breathing is started within thirty seconds of rescuers reaching her. She coughs up water shortly thereafter and is breathing on her own by the time the ambulance arrives.
When found, she has a pulse, but is not breathing. Rescue breathing is started within thirty seconds of rescuers reaching her. She coughs up water shortly thereafter and is breathing on her own by the time the ambulance arrives.
This is the outcome I’ve written. Would this be correct?
A couple of days in the hospital for observation. She’s a princess so they insist on whatever tests CAN be done even if they normally wouldn’t be (X-ray, CT to check brain function.)
Neurologist tells the family that given the length of time in the water, how quickly she was given CPR, and the total length of time not breathing, she will likely suffer only minor cognitive issues at worse, and those may will not present until she starts school.
I’m presuming oxygen via nasal cannula or mask as well as an IV started in the ER.
This does not take place in the US, but I’m presuming standard procedure would be an investigation to find out how she ended up unattended long enough to make it to the waterfront. It’s truly an accident– the first time the child escaped from the house. Is this acceptable? Particularly if there was supporting video evidence?
Jordyn Says:
The scenario you have outlined is reasonable.
Here are a few of my thoughts.
This is a patient we would probably admit into the hospital– at least for a day. More depending on what happens in the first twenty-four hours would determine the need for a more lengthy stay.
For instance. as long as the child has an oxygen requirement with this type of mechanism, they can’t go home. Even if they have normal oxygen levels, any type of increased work of breathing would also probably keep them in the hospital until that resolved. However, if the child’s oxygen levels are normal and they exhibit no signs of respiratory distress for twenty-four hours then we might be hard pressed to keep them in the hospital. Remember, you have to be really sick to stay in the hospital these days.
Of course, with her position as princess, it could be easily foreseen that everyone operates with a greater degree of caution.
Chest x-ray would be reasonable and expected in this case. Paramedics starting an IV and oxygen, particularly in the case where the child received rescue breathing, also good. However, one of the first things that will happen when the child get’s to the hospital is that we will remove the oxygen to see where she settles out on room air. This would be an important piece for us to know. She’d be placed on an oxygen and heart monitor with frequent assessments of her breathing.
As far as doing other testing, particularly a CT scan to determine if there’s been any brain damage, I would argue against this. Now, do physicians “cave” sometimes to pressure by royalty. Of course— I’m sure this has happened. Just as here, if it were the president, some testing might be done that might not be necessary to “cover your . . . “.
Medically, however, if she never lost her pulse and was quickly revived, I think the risk of brain damage is extremely low. As long as your heart is beating, your brain is receiving some oxygen. Your blood does have a reserve volume of oxygen molecules on your blood cells for situations just as this. Children are very oxygen sensitive, and it doesn’t take long for them to lose their pulse in an oxygen deprived state. Knowing she still had a pulse when she was pulled from the water, especially considering her age, would mean to me that her down time was probably very little.
Also, the CT scan will likely not show any injury. Absence of injury also doesn’t mean she may not have learning difficulties in the future. So, I don’t think there’s much to be gained by that test— and the subsequent exposure to radiation which is something we balance a lot in pediatrics.
As far as the investigation, I think what you outline is reasonable, particularly if there is supporting video evidence of her slipping from the castle.
Thanks so much for your question. Good luck with your story!

 come-true via a hyper advanced virtual reality program. The participants receive an implant that allows them to interact virtually with a program partly of their design.
come-true via a hyper advanced virtual reality program. The participants receive an implant that allows them to interact virtually with a program partly of their design. However, medically, this man would have already been dead because they are not providing for either hydration or nutrition. This could be solved simply medically by inserting a feeding tube via his nose and providing free water interspersed with bolus liquid feeds. After all, thousands of people live in comatose states for years if their basic medical needs are met such as oxygen (if needed) and nutrition.
However, medically, this man would have already been dead because they are not providing for either hydration or nutrition. This could be solved simply medically by inserting a feeding tube via his nose and providing free water interspersed with bolus liquid feeds. After all, thousands of people live in comatose states for years if their basic medical needs are met such as oxygen (if needed) and nutrition. In episode 2, the producers must have gotten some feedback that they needed some actual medical equipment if they were concerned about these clients suffering medical complications. This time, a woman’s heart is going into erratic rhythms, specifically V-tach, because of the stress she’s under in her dream scape. But the medical equipment must make sense. What’s pictured in the photo to the right is what we call a rapid fluid infuser. It delivers IV fluids very quickly. Typically, it would be used in a trauma patient or one who is suffering from overwhelming sepsis where rapid delivery of IV fluids can be lifesaving. It is not appropriate for this patient who is suffering from a heart arrhythmia— much better to park a defibrillator at her bedside.
In episode 2, the producers must have gotten some feedback that they needed some actual medical equipment if they were concerned about these clients suffering medical complications. This time, a woman’s heart is going into erratic rhythms, specifically V-tach, because of the stress she’s under in her dream scape. But the medical equipment must make sense. What’s pictured in the photo to the right is what we call a rapid fluid infuser. It delivers IV fluids very quickly. Typically, it would be used in a trauma patient or one who is suffering from overwhelming sepsis where rapid delivery of IV fluids can be lifesaving. It is not appropriate for this patient who is suffering from a heart arrhythmia— much better to park a defibrillator at her bedside. I’m writing about a fifteen-year-old boy who is being abused physically and sexually by his father. One day at school, he tries to commit suicide by slitting his wrists. He becomes scared by the amount of blood, so he leaves the restroom to try to find help. He is found by his teacher and passes out. Now, I know with any kind of suicide attempt, the police are always contacted, and given the all clear for the paramedics.
I’m writing about a fifteen-year-old boy who is being abused physically and sexually by his father. One day at school, he tries to commit suicide by slitting his wrists. He becomes scared by the amount of blood, so he leaves the restroom to try to find help. He is found by his teacher and passes out. Now, I know with any kind of suicide attempt, the police are always contacted, and given the all clear for the paramedics. Flatliners centers around a group of medical students who become curious with the phenomenon of near death experiences (NDEs) to the point that they “flatline” one another so that they can purposefully have one.
Flatliners centers around a group of medical students who become curious with the phenomenon of near death experiences (NDEs) to the point that they “flatline” one another so that they can purposefully have one.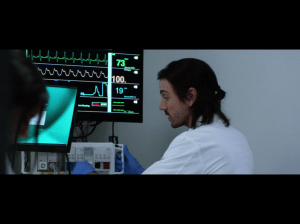 Ray: “The protocol of actually living in the real world. Where guys with crappy HMO’s go undiagnosed with spinal injuries.”
Ray: “The protocol of actually living in the real world. Where guys with crappy HMO’s go undiagnosed with spinal injuries.” Attending: “What is it?”
Attending: “What is it?” Sadly, we know this reality is not true. The pediatric nurse understands and confronts this reality more often than most. Particularly nurses who work critical care, ER, oncology, and hospice.
Sadly, we know this reality is not true. The pediatric nurse understands and confronts this reality more often than most. Particularly nurses who work critical care, ER, oncology, and hospice. I have two scenarios in a novel I’m writing that I could use your help with.
I have two scenarios in a novel I’m writing that I could use your help with.