Holly Asks:

When a patient is in the ICU being monitored, are there warning signals (ie beeping noises from machines to alert, etc) right before or after a person has a stroke? In other words, can it come on suddenly and how does the nurse know it’s happening or has happened?
Jordyn Says:
This is a great question. What exactly can a monitor do and not do for a nurse?
When I was still in nursing school, I did an internship in an adult ICU. At first, I would go running to every alarm and, often times, the nurses would stay at the station and analyze what was happening. Then, I never went into the patient’s room and one day– all the nurses went running to help a patient suffering a lethal rhythm. Discerning what is and is not a patient emergency is a learning curve for every healthcare provider and the monitor should be a tool in the toolbox and not the ultimate decision maker.
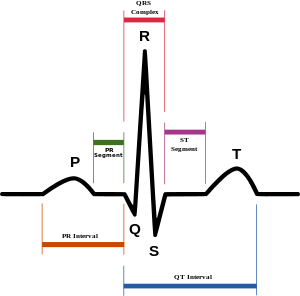
Generally, when a patient is admitted to the ICU, they are placed on cardiac monitoring. This generally includes an ECG (the heart rhythm), the placement of the chest leads will provide a rough count of breathing (through movement of the chest wall as detected by the leads) and oxygen level (which is the lighted probe placed to a finger.)
These are the basics.
All ICU monitoring systems have a tiered alarm system. Meaning, each heart arrhythmia (and other things) are not treated with the same severity. For instance, a heart rate that falls outside the preset parameters may cause the monitor to signal a repetitive single beep or other tone. A good example of this in pediatrics might be a kid whose heart rate increases due to fever and speeds up outside the preset zone.
When a patient goes into a lethal rhythm, like v-fib, v-tach or asystole, the monitor will triple tone.
A stroke is a brain event. Either bleeding, a clot or ischemia causes the patient to lose certain neurological functions that may include speech, and function of a limb. ONLY if these symptoms were precipitated by other vital sign changes (perhaps a drop in oxygen level due to poor breathing) would the monitor alarm. A stroke may not present with a lethal heart arrhythmia. I think a patient would have to signal a nurse that they are experiencing these symptoms or the nurse may discover the patient has suffered a stroke at a scheduled assessment.
However, if the patient is seizing as a result of the stroke, this could cause the monitor to alarm. The seizure motion shakes the leads and it can resemble v-fib on the monitor even though the patient may still be in a normal rhythm but the monitor doesn’t know the difference so it will alarm.
So, I would say it is possible for a patient to suffer a stroke without the monitor alarming.
**************************************************************************

Holly Michael has been published in various national magazines, local newspapers, and in Guideposts books. She also worked as a journalist and features writer. Recently, she signed a contract with Harvest House for a devotional book she’s writing with her son, a type one diabetic in the NFL. Holly lives in Kansas City with her husband, who is an Anglican Bishop. She blogs at http://www.writingstraight.com/ Visit her author page at https://www.facebook.com/AuthorHollyMichael










{kind=link}
{kind=link}